
Accelerate your ACL Rehab in the first 4 weeks
350,000 ACL surgeries injuries occur every single year, with over 1 million worldwide. In America, out of the 350,000 surgeries undergone, statistically, about 105,000 people will re-tear again! This 30% re-tear rate is jaw dropping. Meanwhile only 55% of patients following an ACL injury will return to their pre-performance level.5 One reason these numbers are so devastating is due to the lack of consensus on clinical decision making when returning an athlete back to sport. Argumentatively the first month of rehab is one of the most important phases of the rehabilitation process. It is during the first 4 weeks that you lay down a new foundation, develop, and retrain neuromuscular skills, and set the precedent for the entire rehab process. Here is how you can accelerate your ACL Rehab in the first 4 weeks at Revo Physiotherapy & Sports Performance. We know that tackling the following key components of rehab will take you to where you want to go, better, faster, stronger.
Pain management
Managing your pain will be your first & biggest hurdle. The body’s natural response to any trauma is effusion, or swelling. Effusion in the tibiofemoral and patellofemoral joints can result in decreased quadriceps activation, limited range of motion, and can prevent the patient from progression forward with rehabilitation.6
There are several tools & tricks that can help aid with decreased swelling, which will be implemented the very first day following surgery. Furthermore, once the swelling is being managed it is much easier to control pain levels, minimize quad inhibition, progress gait & so much more.
We take swelling & pain management very seriously at Revo. Following each treatment session we offer recovery boots so your body can immediately start preparing for the next session.

2. Minimize quad inhibition
Following ACL surgery the quadriceps demonstrate muscle inhibition, meaning the quadriceps muscle group as a whole does not like to fire, activate, or turn on. This is why quadricep training is initiated immediately after surgery!2
Having asymmetrical quadricep strength is a large deficit seen in many ACL studies and has a significant correlation with retear rates.1 Here at Revo we do not guess or assume that symmetry is present or not present, but instead we measure it. If it is measured it can be managed.
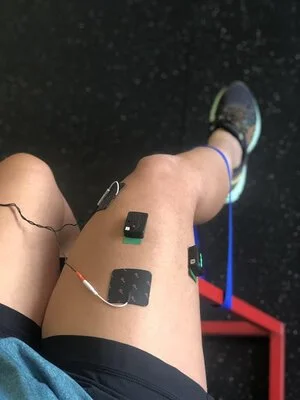
Electromyography is a tool utilized to measure muscle activation. We place sensors on both quadricep muscle groups so we not only can compare side to side but so we can immediately start the facilitating increased neuromuscular pathways from the brain to your affected knee. May people enjoy EMG as they do not feel like it is an exercise but instead like a game.


Neuromuscular stimulation
Through the use of Electromyography we are able to elicit and facilitate increased neuromuscular pathways to the brain. What does this mean? This means that we are helping your brain connect better with your injury & the structures surrounding it. To further fire up the quadricep muscle group and to decrease co-contraction of the hamstring muscle group Neuromuscular Electrical stimulation can be added. NMES combined with exercise was shown to be more effective in improving quadriceps strength than exercises alone.3 Combining this feature with Electromyography can really enhance neuromuscular stimulation just days after surgery.
3. Controlled balance
The earlier you can load that knee the better. A study by Clinical Ortho Related Research found that immediate weight bearing following ACL reconstruction was shown to decrease patellofemoral pain from 35% to 8%.4 For this reason it is imperative to start balance or gait training immediately following your surgery (Unless surgical protocol/WB status says otherwise)
As balance is incredibly important due to the fact that increased weight bearing promotes faster healing times it must be started right away & it must be started right! Improperly loading the knee can result in increased pain, poor gait, future risk for re-tear.
Here at Revo we make sure that you load the knee correctly & truly understand the forces you are putting through your body & how your skeletal position dictates those forces.
Our force plate allows us to analyze not only exactly how much force you are placing through both legs but also helps train body positions to maximize your center of mass relationship with gravity (the earth). It is here we train habits, with dual camera views & ground reaction force vectors we recreate the neural pathways to promote a hip dominant approach to movement rather than a quad dominant position.
You will become a body expert knowing exactly what positions to avoid & more importantly exactly what positions maximize efficiency & performance.


4. Controlled gait
The ability to restore proper gait mechanics following ACL reconstruction surgery is crucial. Before we run, we must walk. For us here at Revo, as we plan to get you back to running as quickly & safely as possible this means we must accomplish perfect walking, as quickly and safely as possible.
We utilize our gait analysis technology to optimize joint kinematics & angles to be sure that each phase is properly executed. Identifying abnormalities in the gait cycle is critical within the first 4 weeks to properly identify and execute proper therapeutic interventions. One of the worst things an individual can do is obtain an abnormal gait pattern, thus causing issues at the ankle, hip, and therefore impeding our overall knee rehabilitation.
5. BFR - Blood flow restriction training
The loss of muscle strength and presence of atrophy is a byproduct of any surgery, especially that of ACL Reconstruction. Regaining that muscle strength & promoting hypertrophy is a priority in not only returning to everyday life but it is critical in returning to sport. It is a well accepted fact that in order to build muscle back, and promote hypertrophy high load training is required. This is the concept of utilizing heavy load resistance training of at least 70% of an individual's 1-rep max.
The caveat here is that following ACL reconstruction surgery, an individual is months & months away from being able to safely load their knee at 70% their 1RM. So what if we could do so early? Say, as early as the first week?! Well, WE CAN.
Blood flow restriction training, a relatively new concept in rehabilitation and has demonstrated that hypertrophic strength gains can be achieved with vascular occlusion. BFR utilizes a special tourniquet system to reduce vascular inflow and completely occlude venous outflow in the limb. This means that we can recreate the hypoxic environment your body would be going under as if you were lifting 70% of your 1RM, but we do so with as little as 20-30% your 1RM, much safer for the post surgical limb! In the short, we can immediately cease the atrophy component of post-surgical repair by executing normal rehabilitation exercises, ie. quad sets, clam shells, single leg balance, partial squats, with Blood Flow Restriction added.
Several clinical studies have taken traditional ACL rehabilitation exercises with the combination of Blood Flow Restriction Training compared to the same exact exercises without Blood Flow Restriction and the differences are remarkable. Takarada et al. 2012 found that the application of BFR for 2-weeks after ACL surgery reduced atrophy in the quadriceps by greater than half compared to those not utilizing BFR.7 Another study by Ohta 2003 looked at the effects of BFR form weeks 2-16 post surgery and found that the BFR group was able to restore quadriceps strength to 91% of the pre-operative level compared to only 64% in the standard of care group.8
6. Faster, Better, Stronger
The first 4 weeks of your ACL rehabilitation are both tough & critical. To truly accelerate your ACL rehabilitation it is paramount that you execute the right pain management techniques, setting you up for optimal recovery. Maximizing quadricep activation through neuromuscular Electromyography training, combined with minimizing quadricep atrophy through blood flow restriction training are just some of the many ways we here at Revo plan to maximize your recovery & minimize your re-injury rate. Faster, Better, Stronger, is the goal and just in the first 4 weeks we embody that vision.
References:
Grindem H, Snyder-Mackler L, Moksnes H, Engebretsen L, Risberg MA. Simple decision rules can reduce reinjury risk by 84% after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804-808. doi:10.1136/bjsports-2016-096031
Lewek M Rudolph K Axe M, et al. The effect of insufficient quadriceps strength on gait after anterior cruciate ligament reconstruction. Clin Biomech. 2002;17:56-63. [PubMed] [Google Scholar]
Effects of Neuromuscular Electrical Stimulation After Anterior Cruciate Ligament Reconstruction on Quadriceps Strength, Function, and Patient-Oriented Outcomes : A Systematic Review Kyung-Min Kim, Ted Croy, Jay Hertel, and Susan Saliba Journal of Orthopaedic & Sports Physical Therapy 2010 40:7, 383-391
Tyler TF, McHugh MP, Gleim GW, Nicholas SJ. The effect of immediate weightbearing after anterior cruciate ligament reconstruction. Clin Orthop Relat Res. 1998;357:141-148. [PubMed] [Google Scholar]
Davies GJ, McCarty E, Provencher M, Manske RC. ACL Return to Sport Guidelines and Criteria. Curr Rev Musculoskelet Med. 2017;10(3):307-314. doi:10.1007/s12178-017-9420-9
van Grinsven S van Gingel REH Holla CJM, et al. Evidence-based rehabilitation following anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2010;18:1128-1144. [PubMed] [Google Scholar]
Takarada, Yudai, Haruo Takazawa, and Naokata Ishii. “Applications of vascular occlusions diminish disuse atrophy of knee extensor muscles.” Medicine and science in sports and exercise 32.12 (2000): 2035-2039.
Ohta H, Kurosawa H, Ikeda H, Iwase Y, Satou N, Nakamura S. Low-load resistance muscular training with moderate restriction of blood flow after anterior cruciate ligament reconstruction. Acta Orthop Scand. 2003;74(1):62-68. doi:10.1080/00016470310013680
Notes:
Quadriceps atrophy is common in an acute surgical knee and can lead to difficulty with active terminal knee extension during gait activities. Quadriceps training is initiated immediately after surgery with isometric quadriceps sets in terminal extension. As tolerated, quadriceps strengthening is progressed to short-arc, open-kinetic-chain strengthening from 308 to physiological terminal extension to aid with normal restoration of gait mechanics. The short-arc quadriceps exercise is shown to activate all quadriceps muscles at a greater EMG level